

Introduction
In recent years, brachytherapy has been considered for brain tumors and is used in many large neurosurgery centers [1, 2]. In this treatment, 125I seeds with activity between 10 and 20 mCi are used. Brachytherapy is an accepted treatment for the treatment of choroidal melanomas to preserve the globe, vision, and quality of life. For the 125I plaque, 20 to 24 seed sources are used, and each seed has an activity of 4 to 6 mCi [3]. Brachytherapy of the prostate with 125I seed is the standard radiotherapeutic approach and is increasing in importance [4–7].
Cattani et al. [4] state that the radiation exposure to the patient’s relatives is below the legal threshold. Several studies have focused on studying occupational doses related to the implant of 125I seed during prostate implants [5–8]. The dose equivalent Hp(10) and Hp(0.07), of less than 30 and 420 μSv per application were measured during prostate brachytherapy with 125I seed [5]. Schiefer et al. [8] studied the radiation exposure of the physician during prostate seed implantation. However, there are few studies to determine the trend in occupational doses received from the 125I ocular plaque during brachytherapy procedures [9, 10]. Al-Haj et al. [9] determined the occupational doses of 125I ocular plaque received during the procedure and compared them with other published data.
Souza et al. [11] evaluated the risks to which workers are exposed during the production and handling of the 125I seed sources. Despite the extensive studies mentioned above, little research has been done on the occupational doses received by the eyes and head skin during the 125I seed implantation procedure. For occupational exposure, the revised equivalent dose limits for the lens of the eye are 20 mSv in a year. Thus, continuous review of eye lens doses of the workers during medical procedures is recommended [12, 13]. The 15 mSv limit has been considered adequate for protection against deterministic effects, although there is some consideration being given at present to reducing this limit in light of more information on visual impairment [14]. Publications from the International Atomic Energy Agency (IAEA) [12], International Organization of Standardization [15], and International Radiation Protection Association [16] recommend routine monitoring above 5 or 6 mSv per year. However, consistent with the as low as reasonably achievable (ALRARA) principle, doses should always be minimized as much as possible. Dose assessment using physical phantoms has been carried out for quite some time in brachytherapy.
In recent years, 125I brachytherapy sources have been used for brain tumors and the treatment of choroidal melanomas in our country using home-made 125I seed [3]. However, our experience during the quality control of 125I seed and the seed implantation during the treatment procedure has shown that there is occupational exposure to the head and neck area, and the radiation protection design is required. Therefore, a computational phantom (VIP-Man model) [17] has been used for dose determination purposes in the head and neck organs, particularly for the eye lens. In the field of safety, handling 125I seed and implantation of seed can be a new approach.
In this study, the primary aim is to evaluate the absorbed dose values of personnel during quality control of low dose rate (LDR) seed sources as well as the dose delivered to the nurse and the physician during 125I seed implantation, such as treatment of a brain tumor or ocular tumor. Furthermore, we demonstrate that the computational method can be used as a reasonable and cost-effective alternative, compared to the experimental approach and the use of the thermoluminescent dosimeter (TLD) and Alderson-Rando phantom for validation of the Monte Carlo (MC) computational model.
Materials and Methods
1. Radioactive Source, Phantom, and Dosimeter Specifications
The 125I seed source is a proprietary product, and its dosimetric parameters were measured by two groups in accordance with the American Association of Physicists in Medicine Task Group no. 43 (AAPM-TG-43) formalism [18, 19]. It was encapsulated by titanium (4.7 mm in length, 0.8 mm in outer diameter, and 4.54 g/cm3 in density) by 15-W Nd:YAG laser welding. The activity of the brachytherapy seed was measured using a dose calibrator (CRC-15BT; Mirion Technologies), which was 15.4 mCi.
An Alderson-Rando phantom is used for the experiment setup. This phantom is proportionally equivalent to an average human with a height of 1.75 m and a weight of 73.5 kg, which is equivalent to tissue. The phantom is cut to a thickness of 25 mm, and each phantom contains a matrix of 5 mm-diameter holes.
A TLD or Perspex chip (Jumei Acrylic Manufacturing Co., Ltd.) equivalent to tissue can be placed in each cavity. We used LiF:Mg, and Ti (TLD-700) chips to monitor the organ dose. The TLD-700 (6Li is 0.01% and 7Li is 99.99%) is used to measure the dose of gamma rays with dimensions of 3 mm×3 mm×0.9 mm [20]. This study employed the method of annealing and reading TLD chips described by Meigooni et al. [21]. The absorbed dose for each TLD is determined by the following equation:
where D is the amount of absorbed dose, R is the amount of the reader output, ECC is the correction factor of the TLD chip, CF is the calibration factor of each TLD, EF is the energy correction factor for the source, RL0 is the average value of Reference Light measured between TLD readings, and RL is the average value of reference light measured between TLD readings of which RL is 94.91. Finally, the background dose is subtracted from the dose that was obtained.
For calculating of dose, the VIP-Man head and torso phantom was used, which was created from transverse color photographic images [22]. Radiosensitive organs, such as the red bone marrow, have been segmented and labeled in the VIP-Man model for dose calculations. This phantom covers the portion of the body from the middle of the lungs to the top of the head. The voxel size is 4 mm×4 mm×4 mm. We use a lattice-based geometry. The input deck is quite descriptive, and we can run it on a Windows system.
2. Experiment Design
To determine the occupational dose in the handling of 125I seed this scenario was considered. LDR seeds for brachytherapy implants have been handled at distances between 5 and 35 cm, which correspond to 20 to 50 cm from the center axis of the phantom. Therefore, the 125I seed was placed at 20 and 50 cm distances from the central axis of the Alderson-Rando phantom in the experimental work. The organ doses were measured by placing TLDs in various parts of the phantom. The sample preparation of TLDs was as follows. In each section, 27 TLDs were utilized. Four TLDs were placed in layer no. 15 of the Rando phantom in front of the chest muscle tissue, three TLDs in layer no. 14 in the lung area, two TLDs in layer no. 12 on the inner surface of the skin. One TLD in layers no. 10 and three TLDs were placed in layer no. 9 in the thyroid area, three TLDs in the right eye area, three TLDs in the left eye area, and finally, five TLDs were placed on the layer of the outer surface of the skin. In order to put TLDs on the eyes and outer surface of the skin, they were first placed in a thin plastic bag and then attached to the phantom. Furthermore, we employed three TLDs as a background control in each step of the experiment. The axis of the seed source was considered at a distance of 20 cm from the central axis of the Rando phantom. This distance was equal to 4.5 cm from the nose tip of the phantom. The steps mentioned in the second section were exactly repeated and only a 50 cm distance was taken into account. Fig. 1 shows the picture of the Alderson-Rando phantom and the location of the TLD on the head and neck, and Fig. 2 shows the location of the TLDs into the torso portion layer. TLDs were placed in different layers of the Alderson-Rando phantom on the thyroid, lungs, eyes, and inner surface of the skin. The irradiation time was set at 20 hours and the TLD dose in each case was obtained using the mentioned method.
3. Monte Carlo Simulation
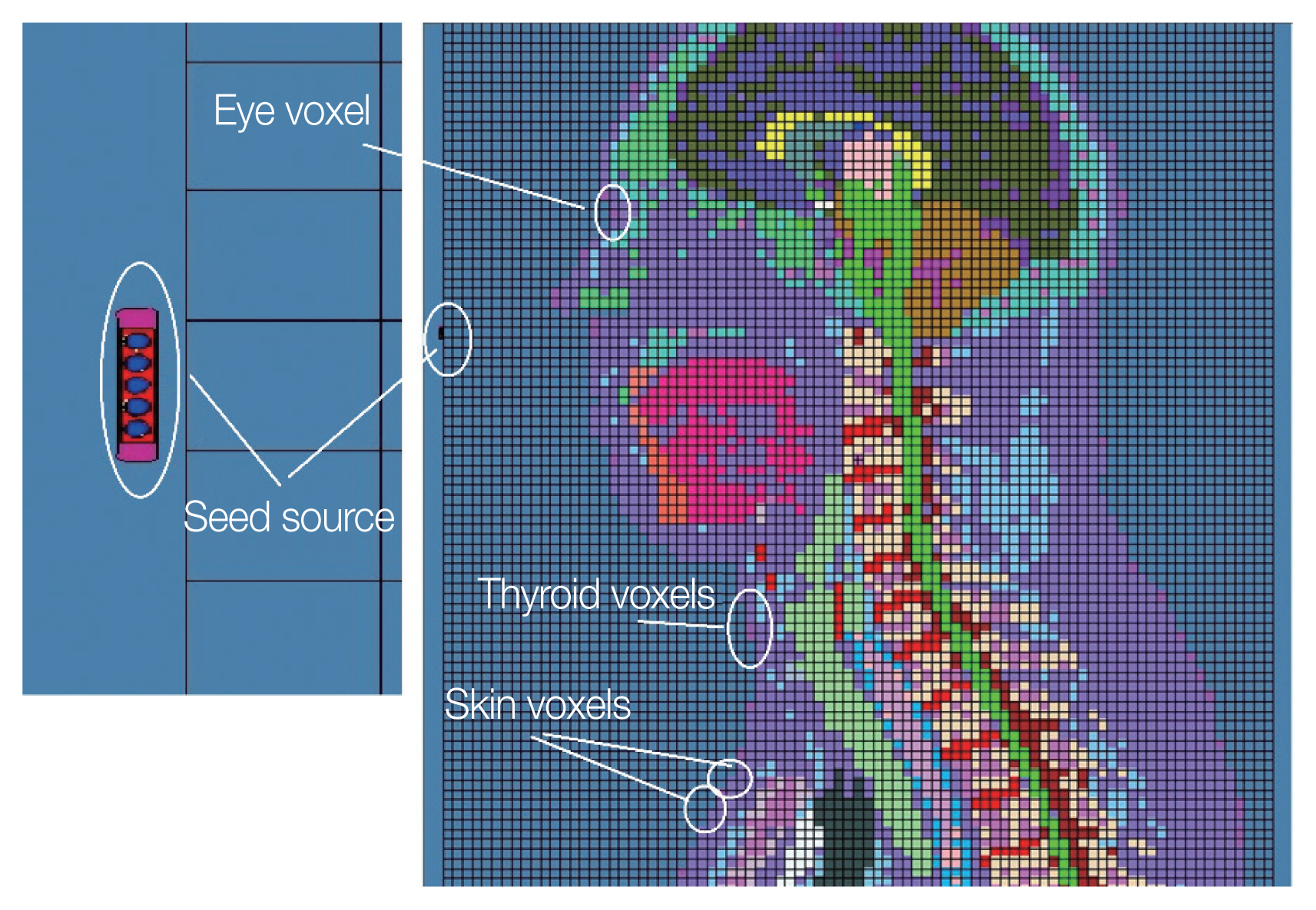
The MC simulations are carried out using the Monte Carlo N-Particle Extended (MCNPX 2.6.0) code, and Evaluated Nuclear Data File (ENDF)/B-VI cross-section libraries were used to simulate the particle interaction [23]. The several application fields of this code include medical physics, radiation protection, and dosimetry. The simulations with default parameters for the transmission of photons and electrons are done. To calculate organ doses, the VIP-Man phantom consisting of predefined organs is used. In the first step to validating MCNPX 2.6.0 code, modeling of the voxel phantom and defining the 125I seed were done based on the geometry between the seed source and the TLD loaded in the computational phantom was used in this simulation. For the two mentioned distances, i.e., 20 and 50 cm from the central axis of the computational phantom, the MCNPX 2.6.0 run was conducted. An image of the computation modeling in X-section (sagittal view) executed with the MCNPX 2.6.0 code is shown in Fig. 3. On the right side of this image, an 125I seed was defined as containing and five resin spheres (5 mm in diameter) with a radioactive spherical layer and a cylindrical of titanium capsule (4.7 mm in length, 0.8 mm in outer diameter, and 4.54 g/cm3 in density). The distance between the central axis of the seed and the central axis of the computational phantom was defined as 20 cm. The output from the MC calculation, was computed using the *F8 energy deposition tally in units of MeV/photon from the mesh tally and 8×107 number of histories. Finally, dose rate was calculated in units of cGy/mCi/hr. To perform more comprehensive dosimetry for different positions of the source from the central axis of the phantom, such as 20, 30, 40, and 50 cm, the MCNPX 2.6.0 code was run in the next step.
Results and Discussion
Table 1 displays the comparison of the MCNPX 2.6.0 dose results with the results of the TLD experiments for validating the MC simulation. The quantity of external irradiation caused by handling 125I seed is shown by the dose values for the organs, which are shown in mGy. The statistical uncertainties (type A) due to repetitive TLD measurements are found to be 7%, 4%, 4%, and 16% for the eye, thyroid, lung and skin respectively. The uncertainties (type B) due to dose calibration and TLD positioning are found at 5% and 5% respectively. The total uncertainties for this dosimeter are calculated as 10%, 8%, 8%, and 18% for the eye, thyroid, lung and skin, respectively. Table 1 presents the uncertainties for the absorbed dose.
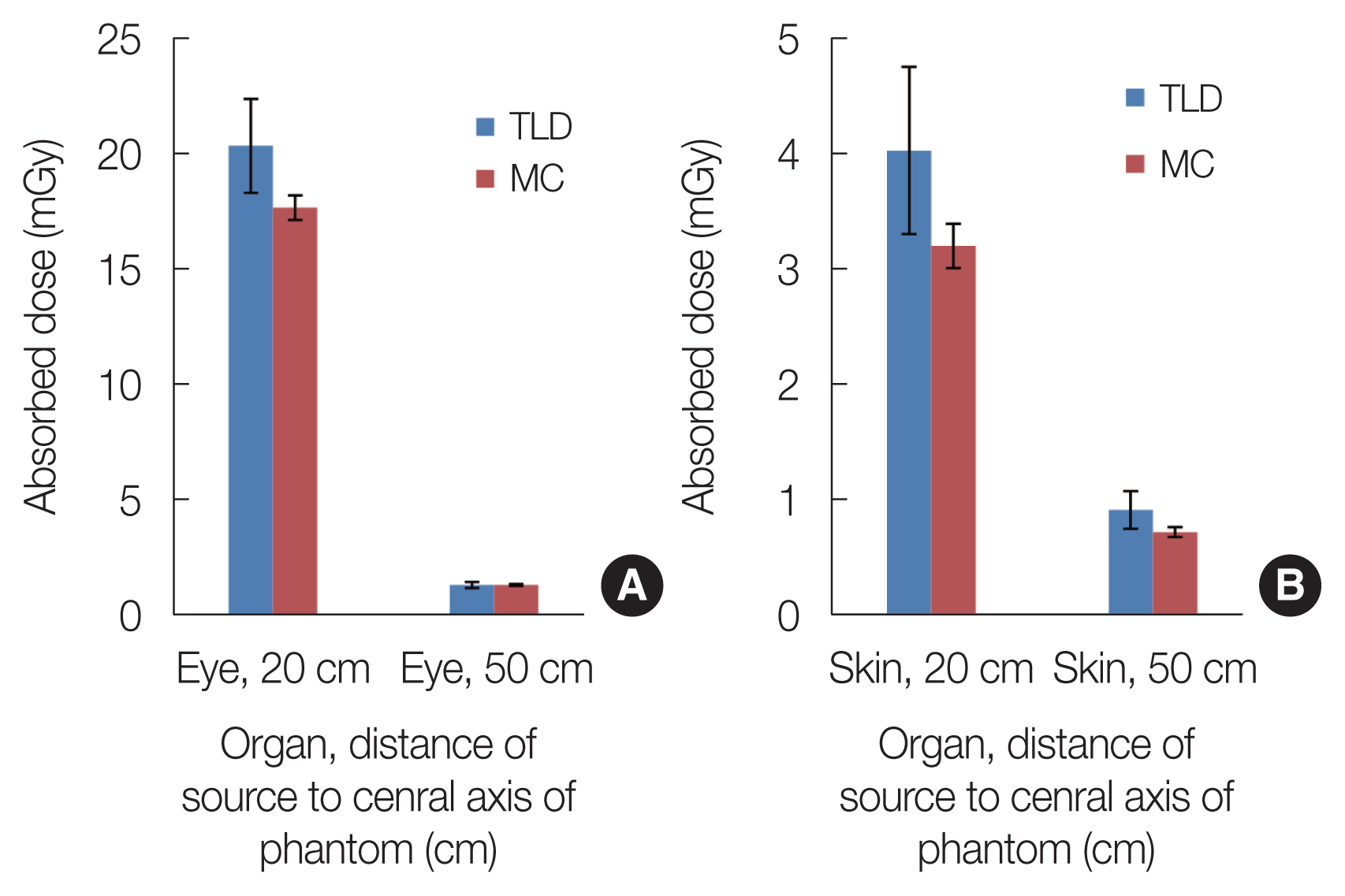
As can be seen, the experimental results and the values derived from MCNPX 2.6.0 in the thyroid and lung organs are consistent. However, the relative difference of MC dosimetry to TLD for the eyes is between 4% and 13% and for the skin between 19% and 23%. Fig. 4 shows the comparison of the absorbed dose for eye and skin using the TLD and MC methods and their uncertainties. Due to the higher uncertainty for TLD in eye and skin, as depicted in Fig. 4, these relative inaccuracies can be tolerated. The main reason for this relative difference could be due to the difference in the position of the TLD inside the Alderson-Rando phantom relative to the computational head phantom.
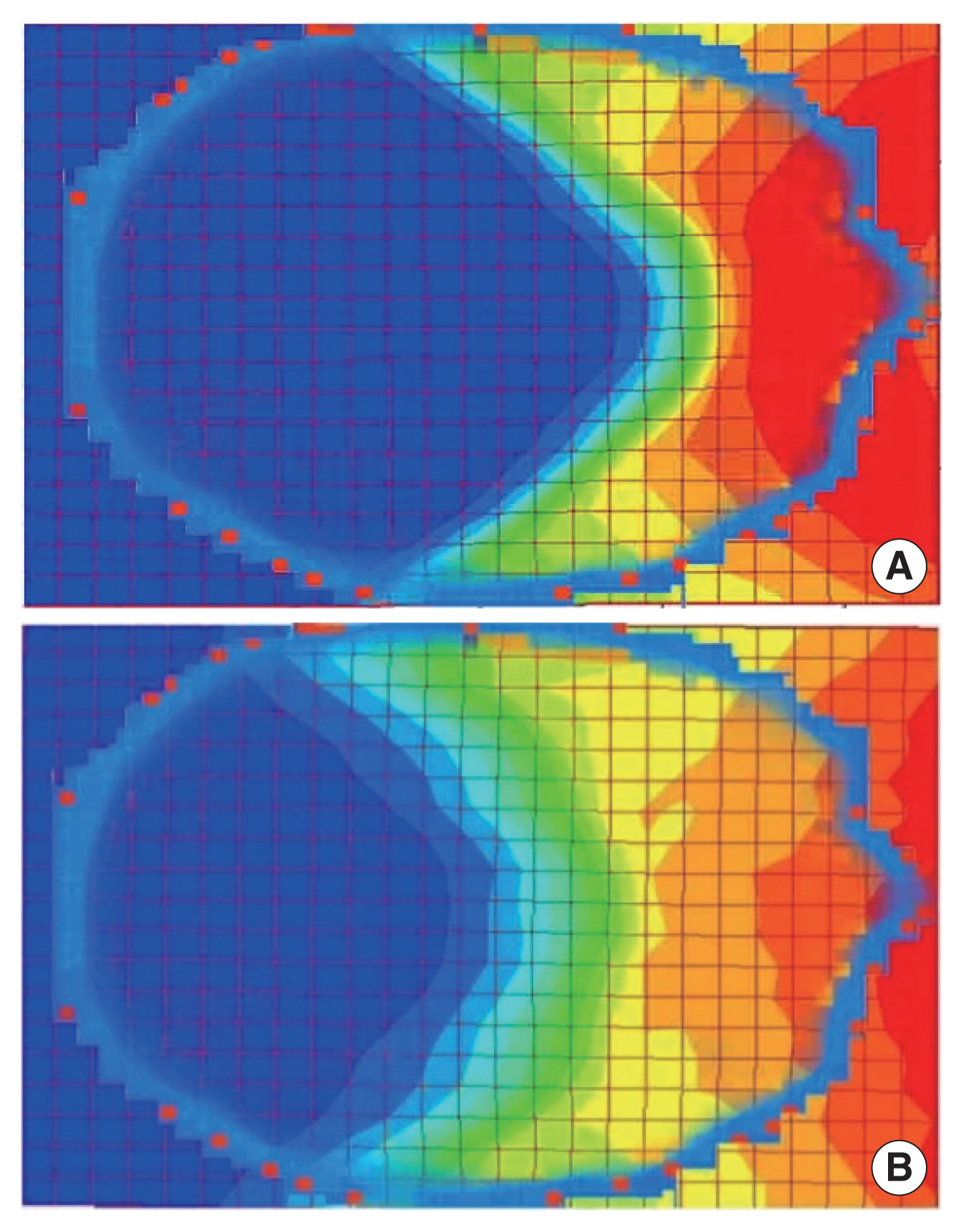
The diagram of the absorbed dose rate in grayscale levels and isodose obtained from the MCNPX 2.6.0 when the 125I seed was placed at two distances of 20 and 50 cm from the central axis of the phantom is shown in Fig. 5. This diagram shows a Z cross-section (transverse plane) of the head phantom, which can be seen on the right side of the eye and nose cross sections. The value of each voxel is in cGy/hr per source particle. We use Tec-plot software (Tecplot Inc.) to draw isodoses. The red pixels show the areas with the highest dose (hot spots), and the blue pixels show the areas with the lowest dose. The greatest dose reduction is observed for the eyes, skin, thyroid and lungs, respectively. The results show that a 30 cm displacement for the 125I seed reduces the eye dose and skin dose by at least about 12 and 4 times, respectively.
For occupational dosimetry purposes, the 125I seed was placed at a distance of 20, 30, 40, and 50 cm from the VIP-Man phantom. The calculated dose rates in terms of μGy/mCi/hr are given in Table 2. According to the results, we observed that the eye lenses receive the highest dose, followed by the skin layer, the thyroid, and finally the lungs. If there are no lead glasses on the eyes, the maximum exposure time of 125I seed (activity of 15.4 mCi) can be estimated. Therefore, the maximum working time according to the weekly occupational limit, 1 mSv/week, will be about 1.2 and 13.4 hours for 20 and 50 cm distance, respectively.
Anglesio et al. [5] recorded the doses equivalent Hp(10) and the equivalent dose Hp(0.07) of less than 30 and 420 μSv using film and finger ring dosimeters during brachytherapy with the 125I seed. Kaulich et al. [6] reported Hp(0.07) values up to 1 mSv on the hands. In Table 1, we also reported a skin dose of about 298 μSv (for a time of 2 hours and a distance of 20 cm), which is in agreement with those reported by other authors for the finger dose. The use of lead gloves reduces the dose to the hands, and a reduction of about 50% in the received doses was observed.
The equivalent dose at a depth of 0.07 mm, Hp(0.07), using TLD-100 (LiF:Mg, Ti) dosimeters for the physician’s eye during interventional radiology was measured by Bahruddin et al. [13]. They report a mean Hp(0.07) dose of 0.33 mSv and 0.20 mSv for the left and right eye lenses, respectively. The eye lens radiation exposure was recorded in terms of the equivalent dose, Hp(0.07), and the dose under the lead apron was recorded as Hp(10). The effective dose was calculated based on the following equation:
Equation (2), known as the Von Boetticher algorithm, was derived based on International Commission on Radiological Protection 103 [13].
The IAEA recommended that for the mean photon energy below about 40 keV, Hp(0.07) may be used but not Hp(10). For non-homogeneous radiation fields, monitoring near the eyes is necessary. When protective equipment such as lead glasses is in use, monitoring near the eyes and below the protective equipment or an equivalent layer of material is necessary. Otherwise, appropriate correction factors to take the shielding into account should be applied. If a lead apron is used for the trunk, monitoring below the shielding underestimates the dose to the lens of the eye as the eye is not covered by the trunk shielding. However, separate monitoring near the eyes is necessary [14].
Quantifying the protection provided by lead glasses is difficult, and most dosimeters are not designed to be used under lead glasses [24]. In this study, we introduced a method to determine the absorbed dose for eyes (without lead glasses) using a computational phantom. It can be used to monitor the dose to the eye for personnel involved in the handling of 125I seed. This data can be useful for designing the thickness of lead glasses suitable for working with 125I seed.
Conclusion
The absorbed dose values for eyes, eye lens, thyroid, skin, and lung were evaluated using a computational phantom during the handling of 125I seed. The TLD and the Alderson-Rando phantom were used to validate the MCNPX 2.6.0 code. The two-dimensional diagram of the absorbed dose rate in grayscale levels shows that the eye lenses and eyes receive the highest dose. Therefore, there is a need to move the source or reduce time, which was quantitatively evaluated in this study. The results indicated that for near the head (distance of 20 cm) the absorbed dose rate for the eye lens, eye and skin were 78.1±2.3, 59.0±1.8, and 10.7±0.7 μGy/mCi/hr, respectively. Additionally, we found that a 30 cm displacement for the 125I seed reduces the eye and skin doses by at least 3- and 2-fold, respectively. For future studies, a computational phantom can be utilized to monitor the dose to the eye and skin of personnel who are equipped with protective devices (such as lead glasses and an apron).