

Introduction
The Fukushima Daiichi Nuclear Power Plant (FDNPP) run by the Tokyo Electric Power Company (TEPCO) was damaged by the Great East Japan Earthquake and subsequent massive tsunami on March 11, 2011, which led to a serious nuclear accident with an enormous release of radioactive materials into the surrounding environment [1]. More than 8 years have passed since this accident; however, there remain areas where the ambient dose rates are significantly elevated due to the radionuclides deposited on the ground (mainly, 137Cs at present) and a large number of Fukushima residents have been obliged to evacuate from their hometowns.
It is necessary to evaluate the potential radiation exposure doses to persons involved in the FDNPP accident, in particular Fukushima children. Extensive efforts to do so by Japanese experts have been described elsewhere [2]. One consensus view of the relevant studies was that both external and internal doses to residents were expected to be low in general, and thus radiation-induced health problems would not be notable in the future. However, one critical problem that remains is that there are many uncertainties in the estimation of thyroid doses, mainly from the intake of radioiodine that existed only during a short period of time after the accident. The isotope making the biggest contribution to the internal thyroid dose was 131I, with a physical half-life of 8 days, which was also the case in the Chernobyl Nuclear Power Plant (NPP) accident. However, the number of direct human measurements of 131I was very limited in the FDNPP accident.
Fukushima Medical University began performing extensive health examinations for residents, named the Fukushima Health Management Survey (FHMS), at the end of June 2011, on commission from Fukushima prefectural government [3]. The FHMS consists of the Basic Survey (external dose estimations) and the Detailed Surveys. One component of the Detailed Surveys is the thyroid ultrasound examinations performed to detect thyroid diseases as early as possible, targeting approx. 370,000 residents aged 0–18 years at the time of the earthquake. As a result, approx. 200 malignant cases (including suspected malignancies) were found as of December 2017 (http://www.pref.fukushima.lg.jp/site/portal/43-7.html). The Exploratory Committee of the FHMS stated that these malignant cases were unlikely to be caused by radiation exposure because thyroid doses were expected to be much lower than those in the Chernobyl NPP accident. However, the committee also claimed that further studies were necessary to clarify this issue (http://www.pref.fukushima.lg.jp/uploaded/attachment/158522.pdf).
This paper provides a review of the published literature on the thyroid dose estimation, mainly for Fukushima residents, together with additional explanations and a discussion of the relevant problems. Note that the thyroid dose was caused by external radiations as well; however, this was not a focus here because of the relatively small contribution of external exposure compared to internal exposure.
Methods for Estimating Internal Thyroid Doses
This section describes the main methods used for estimating internal thyroid doses in the FDNPP accident. In general, internal dose estimation is more complicated than external dose estimation because the internal dose cannot be directly measured and is associated with many assumptions made by the assessors. The sources mainly used for the internal thyroid dose estimation are two-fold: direct (in vivo) measurements and environmental data.
The direct measurements refer to measurements of radionuclide(s) in the human body using a photon detector placed near the subject [4]. This method is available when the radionuclide(s) of concern emits photons with enough high energy to penetrate the body tissue and an abundant yield. Regarding 131I, the most detectable photon energy line is 365 keV (81.7%). The detector used is typically placed near the front bottom of the neck since iodine is localized in the thyroid. Before the measurements are made, the detector needs to be calibrated using suitable phantoms that mimic the human thyroid and neck [5]. It is noted that direct measurements can tell only the body content (Bq) at the time of the measurement. For the internal dose estimation, reasonable assumptions regarding the intake day(s), the route of intake (inhalation, ingestion, injection), and the physicochemical characteristics of the radioactive materials of concern are essential.
The environmental data available for internal dose estimations are the radioactivity concentrations in air, food and drink items, and so on. However, unfortunately, such data were not adequately obtained during the early period when a detectable amount of 131I existed in the environment. In fact, continuous air sampling was not carried out within Fukushima Prefecture at that time. It was found later that air sampling filters collected by suspended particulate matter monitors installed at many locations to detect air pollutants would be potentially available for the internal dose estimation [6]. However, the exact intake amount is difficult to determine unless other information is obtained, such as the indoor dose reduction factor for airborne radioactive materials, the respiration rate during exposure, the food and drink consumption during emergency situations, the actual effects of radiation protection measures taken by authorities and/or individuals, and so on. In terms of the inhalation of radioiodine, the chemical composition also needs to be determined because the dose coefficients (Sv per Bq intake) differ among its chemical forms: elemental iodine, methyl iodide and particulate iodine. Consequently, the internal dose estimation based on the environmental data is likely to involve considerable uncertainties. On the other hand, information on the chemical composition of iodine is not necessarily required in the dose estimation based on the direct measurements described above. However, it should be noted that such dose estimations also contain uncertainties related to assumed intake scenarios.
In the Chernobyl NPP accident, models of the transfer of radionuclides from the environment to cow’s milk were used to estimate the internal thyroid doses of residents in contaminated territories [7, 8]. These models assumed that the residents continued to consume milk contaminated with 131I for a certain period of time, which was considerably different from the situation in the FDNPP accident. A survey of the food supply system suggested that consumption of the contaminated food and drink items by residents would have been limited shortly after the accident due to prompt countermeasures and the collapse in supply chains in the prefecture [9].
Review of the Relevant Publications
This section provides a brief review of the publications relevant to estimations of the internal thyroid doses to Fukushima residents, in particular the doses in the areas radiologically affected by the accident. Table 1 provides a summary of the dose estimations for children from the publications described below.
1. Estimation from Direct Measurements for 131I
This category provides the most reliable dose estimates; however, the number of measurements was limited. The largest dataset in this category was obtained from the screening campaign by the Nuclear Emergency Response Local Headquarters at the end of March 2011 [10, 11]. This campaign was performed in Kawamata town, Iwaki city, and Iitate village only. Moreover, these three municipalities are located mostly outside of the 30-km radius of the FDNPP, within which either evacuation or sheltering indoors was ordered right after the accident; however, internal thyroid exposure to children living in the areas was expected to be high based on predictions made by atmospheric transport dispersion model (ATDM) simulations. In the campaign, 1,149 subjects were recruited and internal thyroid doses were estimated for 1,080 of the subjects, demonstrating that their doses were much lower than the 100 mSv dose (thyroid equivalent dose) predicted by the ATDM simulations for hypothetical 1-year-old children who remained outdoors all the time. The level of 100 mSv was regarded as a cutoff level in the screening; no measures were supposed to be taken for persons below this level. The results of the assessment of the 1,080 subjects’ thyroid doses were provided in the present authors’ latest paper [11]. As a result, the thyroid doses were less than 30 mSv for most of the subjects.
Tokonami et al. [12] independently performed their measurements during the period from April 12 to April 16, 2011. As a result, 131I was detected in 46 out of 62 subjects from Namie town and Minamisoma city. The median (maximum) thyroid doses to children (under 20 years of age) and adults based on the assumption that they inhaled 131I on March 15 only were 4.2 mSv (23 mSv) and 3.5 mSv (33 mSv), respectively.
Matsuda et al. [13] performed measurements with a whole-body counter (WBC) owned by Nagasaki University. They examined 173 subjects within the first month after the accident. These subjects were mostly evacuees from Fukushima Prefecture and first responders from Nagasaki Prefecture. The average stay period of the subjects in Fukushima Prefecture was 4.8 days. As a result, 131I, 134Cs, and 137Cs were detected in about 30% of the subjects. The maximum thyroid dose (20 mSv) was found in a subject who was categorized in the earliest evacuation group with a stay period of March 11–18. The thyroid dose was much lower in subjects who had stayed in Fukushima Prefecture at earlier times.
There have also been a few other reports related to direct measurements of 131I [14–16]; however, the number of subjects examined in each study was very limited. Thus, regarding the general public, the number of people for whom data are available is only about 1,300 in total, which is much less than the number of persons whose thyroid doses should be carefully evaluated (e.g., children, pregnant women, delayed evacuees).
2. Estimation from Direct Measurements for Cesium
Fukushima prefectural government started WBC measurements at the end of June 2011 in order to clarify the levels of internal contamination in residents. These measurements have been continued to the present; the number of measurements has reached 341,430 as of September 2019 (http://www.pref.fukushima.lg.jp/site/portal/ps-wbc-kensa-kekka.html). Details on the WBC measurements conducted in the prefecture have been described elsewhere [17].
Although the WBC measurements targeted 134Cs and 137Cs rather than 131I, relatively early WBC measurements (at least those performed until the end of 2011) could be utilized to estimate thyroid doses by determining an activity ratio of these two elements. Kim et al. [18] derived the intake ratio of 131I to 137Cs by comparing the thyroid and effective dose distributions for residents of Kawamata town and Iitate village at the same upper percentiles (e.g., 80th, 90th, and 95th percentiles). Here the thyroid dose distribution (131I) was obtained from the screening campaign, whereas the effective dose distribution (134Cs/137Cs) was obtained from WBC measurements of adult subjects. The lower percentile or median values for the two dose distributions were not used due to the low detection rates in both measurements. The intake ratio was also introduced based on the assumption that adults and children in the same municipality inhaled 131I and 137Cs with the same activity ratio, but with different respiratory volumes depending on age. As a result, the intake ratio of 131I/137Cs was derived to be 2.4–3.3 for Kawamata town and 2.0–2.3 for Iitate village. Using the derived intake ratio of 3 (as a rounded average), Kim et al. [19] presented estimates of the 90th percentile thyroid doses to 1-year-old children based on the effective dose distributions for adults from several municipalities [19]. The estimate for 1-year-old children was 30 mSv as the 90th percentile value for the relatively high dose areas. A similar approach to this was also attempted for Namie town’s residents by Hosoda et al. [20] and Kim et al. [21], resulting in a large discrepancy in the derived intake ratio of 131I/134Cs: 0.1–0.9 (a geometric mean, 0.2) and 3–5 (average, 3.8), respectively.
One question addressed in these studies is for how long a trace of the early intake remains in WBC measurements. In this regard, it should be noted that the biological half-life of cesium is much shorter in children than in adults. In WBC measurements over the period between June 27 and July 28, 2011, the ratios of subjects with the presence of both 134Cs and 137Cs in adults and children were 28.8% and 4.1%, respectively [21]. An overestimation of the cesium intake is also likely to occur in children based on an acute intake scenario on potentially the earliest day [17]. On the other hand, it has been found that the cesium detection rate tends to be higher in late evacuees from areas near the FDNPP in the case of adult subjects, suggesting that a trace of the early intake would appear in the WBC measurements until about half a year after the accident [22, 23].
3. Estimation from Other Sources
Kim et al. [24] estimated the internal thyroid doses to residents using the results of ATDM simulations and 18 evacuation model patterns. In this estimation, a dose reduction factor due to sheltering indoors was not factored in considering inhalation as an exposure pathway of concern. From direct measurements, the estimated thyroid doses were found to exist around the upper levels of the estimated doses. The United Nations Scientific Committee on the Effects of Atomic Radiation (UNSCEAR) also estimated internal doses from inhalation using other ATDM simulations, but indirectly, by using a ratio obtained in the simulations, namely the relationship between the ground deposition density (GDD) and the time-integrated air concentration [25]. Regarding the GDD, measurement data were available.
Measurement data for the radioactivity in food and drink items were needed to estimate the internal doses from ingestion. The UNSCEAR and the World Health Organization estimated that doses based on conservative assumptions, such as continuing the consumption of contaminated food items for a certain period of time [25, 26]. According to the estimates by the UNSCEAR, the thyroid absorbed doses to infants (1 year of age), children (10 years of age), and adults in Fukushima Prefecture were 32.8 mGy, 15.2 mGy and 7.78 mGy, respectively, only from ingestion. By contrast, Murakami and Oki [27] estimated the thyroid doses from ingestion taking into account the effects of countermeasures (as in the Case 1 scenario): 1.7 mSv (<1 year), 2.1 mSv (7–12 years, male), and 0.84 mSv (≥19 years, male) for citizens in Fukushima city. Kawai et al. [28] also reported the thyroid doses from the ingestion of tap water based on realistic intake scenarios with reconstructed time trend profiles of the 131I radioactivity concentration.
With regard to estimations from other human data, Kamada et al. [29] reported thyroid doses of 27–66 mSv based on the 131I radioactivity in urine samples. 131I was detected in urine in 5 out of 15 subjects (including 4 children) from Kawamata town and Iitate village; only one of the 4 children was positive in his urine sample (44 mSv). Ohba et al. [30] performed a unique dose estimation using the body surface contamination levels of evacuees from areas near the FDNPP. In this study, the intake by inhalation was derived assuming that 131I in air caused body contamination by its deposition during the period when residents were potentially exposed to radioactive plumes. The 90th percentile thyroid doses for 1-year-old children of the Namie group, the Minamisoma group, and the group comprising four municipalities (Tomioka town, Okuma town, Futaba town, and Naraha town) were estimated at 40.1 mSv, 14.8 mSv, and 4.0 mSv, respectively.
Discussion
As shown in Table 1, the internal thyroid dose estimates are different among the studies. The most reliable estimates based on direct measurements for 131I [11–13] were found to be below 20–30 mSv; however, the number of such estimates was limited. The relatively high estimates by the UNSCEAR [25] are, as described earlier, due to basing the ingestion doses on conservative assumptions: 32.8 mGy for 1-year-old children in the whole of the prefecture (excluding the evacuation areas). The estimates by Kim et al. [24], which were also considered conservative in general, differed greatly among the municipalities. These estimates are only for the inhalation dose; however, they are higher than those by the UNSCEAR (including the ingestion dose) in Futaba town and Namie town, whereas they are much smaller in Okuma town and Tomioka town despite the use of 18 similar evacuation model patterns. One critical note in this study is that the evacuation behaviors of residents in the neighboring areas for the first few days after the accident would greatly influence the estimations of their thyroid doses from inhalation. In this context, one should pay attention to the fact that many residents were voluntarily evacuated even from areas where immediate evacuation was not ordered [19, 31], resulting in possibly averting exposure to radioactive plumes that were significant in the first week. According to the UNSCEAR, the thyroid dose averted by prompt evacuation was estimated at 750 mGy for 1-year-old children in the neighboring municipalities [25].
The first comprehensive estimation for Fukushima residents was presented by the authors [32] in January 2013 (later published [19]). This estimation was provided only for about 90th percentile inhalation doses in light of the fact that ingestion doses would have been minimized due to the prompt restriction of the consumption and distribution of contaminated food and drink items [33]. The estimation was mainly based on the effective doses of adult subjects according to WBC measurements and complementarily from ATDM simulations. The latter were applied to areas where direct measurement data were unavailable, such as the Aizu and Nakadori regions (the west and middle areas of Fukushima Prefecture), Iwaki city, and so on. One key factor in this estimation is the use of the derived intake ratio to convert the effective dose to the thyroid dose. It might be considered reasonable that the derived intake ratio of 131I to cesium was much lower than the activity ratio of the two elements in various environmental samples (e.g., 8 for the time-integrated air concentration observed in Ibaraki Prefecture during the period between March 13 and May 23, 2011), taking into account the relatively-low thyroid iodine uptake (TIU) in Japanese populations due to their diet [18]; however, further studies on this matter are necessary.
The recent dose estimations by Ohba et al. [30] and Kawai et al. [28] are provided for the inhalation dose and the ingestion dose, respectively. The sum of these two dose estimates was also mostly less than 20 mSv (at the 90th percentile level) for the municipalities near the FDNPP. However, the 90th percentile thyroid dose of the Namie group reached 46.4 mSv in total (40.1 mSv from inhalation and 6.3 mSv from ingestion), although this value was reduced by two-thirds (30.9 mSv) by taking into account the average TIU value in Japanese populations [30]. A crucial point recognized in recent studies is the date of the first exposure, which is important in terms of the dose contribution from short-lived radionuclides other than 131I. The thyroid dose only from 131I would increase by 1.59 times in the case of exposure to radioactive plumes from March 12–14 (1.09 times for exposure from March 15–17) when taking into account the dose contribution from 132Te-132I and 133I [30]. This has been also pointed out by Shinkarev et al. [34]. In contrast, Kim et al. [19] set the ratio at 1.1 based on the results of continuous air monitoring at a location in Ibaraki prefecture where the first plume arrived on March 15. Our latest study [23] demonstrated that approx. 20% of Namie town’s residents stayed within the 20-km radius of the FDNPP as of 3:00 pm on March 12 or later, and their effective doses were considerably higher than the doses of those who had already evacuated outside the 20-km radius before that time. This result might suggest that late evacuees from the neighboring areas were additionally exposed to radioactive plumes released from Unit 1 which caused the hydrogen explosion on the same day. In that case, the dose contribution from the short-lived radionuclides other than 131I would needed to be carefully evaluated. On the other hand, the dose received on March 15, when the largest release event occurred at Unit 2 is expected to be small because most residents had moved to distant places by that time.
In conclusion, the estimation of thyroid doses to Fukushima residents still has many uncertainties However, although the dose estimates from various studies differ, it is believed that the thyroid doses are unlikely to exceed 50 mSv excluding some extreme cases (e.g., persons who continued to consume highly contaminated items or did not evacuate from areas close to the FDNPP). The dose reduction effects of self-protection measures by the residents might have be significant, judging from the results of the screening campaign in Iitate village where tap water was significantly contaminated with 131I in the early period compared to other areas. Further multilateral studies are thus necessary to reduce the uncertainties in the present dose estimations.
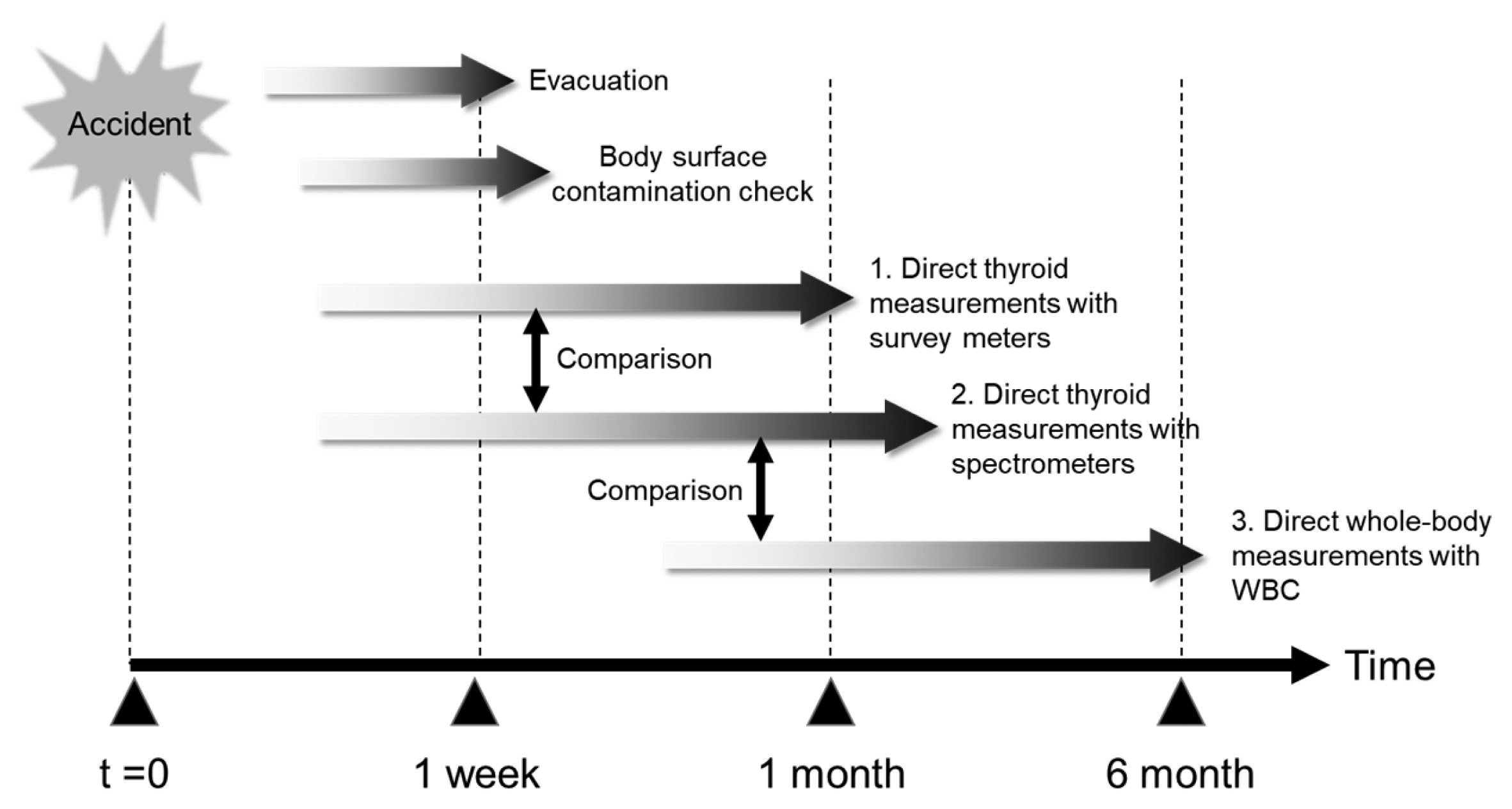
Finally, we would like to describe our proposed method for population monitoring in case of a future nuclear accident based on lessons learned from the experiences of the FDNPP, in particular in terms of the thyroid dose estimation of the public. The outline of this method is shown in Fig. 1. Note that population monitoring is carried out following evacuation of people in the areas designated based on measurement results of the ambient dose rate there. According to the Japanese guidelines for nuclear emergency response stipulated after the FDNPP accident, evacuation criteria are basically operational intervention levels (OILs): OIL1 (500 μSv·h−1) for prompt evacuation and OIL2 (20 μSv·h−1) for protracted evacuation (within 1 week) [35]. These OIL values were arranged from the original values in the IAEA safety guides [36, 37] based on experiences of the FDNPP. The propose population monitoring method is composed of three types of direct measurements to obtain as many human data as possible for the dose reconstruction following a nuclear accident. The first type is direct thyroid measurements with survey meters (non-spectrometric devices), which are basically the same as the screening campaign conducted shortly after the FDNPP accident [10, 11]. The second type is direct thyroid measurements with spectrometric devices and third type is direct whole-body measurements with WBCs. Each type of direct measurements has advantages and disadvantages; however, would be reasonably compensated by comparing with each other. The first type measurements are intended to be performed with a main purpose of triage to identify persons who are heavily exposed. It is assumed that measurers are first responders at each site including non-radiation experts (e.g., local government officers). Survey meters (typically, a NaI(Tl) scintillation probe-type) are easy-to-use devices and suitable for quick measurements. For validation of the first type measurements, the second type measurements may be used by comparisons of the 131I thyroid contents of selected persons who undergo both types of measurements [38]. The second type measurements will provide the most reliable data for the thyroid dose estimation; however, need a longer counting time and adequate training for handling the devices. The third type measurements target 134Cs and 137Cs in contrast to the other two types of measurements. These measurements would be effective for persons who miss early direct measurements if an appropriate value of the intake ratio of 131I/Cs can be determined from the same persons with significant intake of both elements.
Apart from direct measurements of the affected populations, information on their evacuation behaviors should be collected as early as possible. This information will be essential to assume the time of intake of radionuclides together with results of environmental monitoring. The dose contribution from short-lived radionuclides other than 131I should be taken into account if a significant intake event is expected within the first few days after a nuclear accident [34]. Assuming the difficulty in measuring 132Te-132I and 133I in persons, it may be practical that the potential intake of these radionuclides is estimated from the measured 131I thyroid content and the nuclear core inventory. In the first type measurement, it is supposed that a screening level corresponding to OIL8 [37] is determined as a net reading value of the devices used. A relatively-high gamma emission rate of 132I may cause overestimations of the internal thyroid dose if the OIL8 value is derived assuming intake of 131I only; however, this would not be a significant problem.
Further considerations on the proposed method will be reported in the authors’ future publication. However, one thing for sure is, as experienced in the past nuclear accidents, that the number of people to be examined regarding their radiation exposure can be overwhelmingly large. It is thus crucial for each county to establish and maintain a steady and effective population monitoring system as a part of a national-level scheme for radiation emergency response [17].