Dosimetric Comparison of 6 MV Flattening Filter Free and 6 MV Stereotactic Radiosurgery Beam Using 4 mm Conical Collimator for Trigeminal Neuralgia Radiosurgery
Article information
Abstract
Background
The purpose of our study was to compare the dosimetric advantages of Flattening filter free (FFF) beams for trigeminal neuralgia patients using 4 mm conical collimators over previously treated patients with 6 MV SRS beam.
Materials and Methods
A retrospective study was conducted for 5 TN patients who had been previously treated at our institution using frame-based, LINAC-based stereotactic radiosurgery (SRS) on Novalis Tx using 6 MV SRS beam were replanned on 6X FFF beams on Edge Linear accelerator with same beam angles and dose constraints using 4 mm conical collimator. The total number of monitor units along with the beam on time was compared for both Edge and Novalis Tx by redelivering the plans in QA mode of LINAC to compare the delivery efficiency. Plan quality was evaluated by homogeneity index (HI) and Paddick gradient index (GI) for each plan. We also analyzed the doses to brainstem and organ at risks (OARs).
Results and Discussion
A 28% beam-on time reduction was achieved using 6X FFF when compared with 6X SRS beam of Novalis Tx. A sharp dose fall off with gradient index value of 3.4±0.27 for 4 mm Varian conical collimator while 4.17±0.20 with BrainLab cone. Among the 5 patients treated with a 4 mm cone, average maximum brainstem dose was 10.24 Gy for Edge using 6X FFF and 14.28 Gy for Novalis Tx using 6X SRS beam.
Conclusion
The use of FFF beams improves delivery efficiency and conical collimator reduces dose to OAR’s for TN radiosurgery. Further investigation is warranted with larger sample patient data.
Introduction
Trigeminal neuralgia (TN) is an unbearable pain syndrome with an electric-shock like pain in the trigeminal nerve of affected patients. Treatment modality for TN includes medical treatments through drugs, surgical treatment, and radiosurgery treatment. The first line treatment is by medical management using anti-seizure medications. In case if the patient does not respond to medications, surgical treatments including balloon compression, percutaneous rhizotomy, microvascular decompression (MVD) have been used [1–6]. Radiosurgery is also considered as one of the treatment options due to its minimally invasive procedure as reported by Leksell in 1951 [7]. The TN target is considered to be one of the smallest targets for treatment hence it requires a high precision and accuracy radiosurgery unit. The Gamma knife Radiosurgery has been shown to be safe and effective to treat TN [8–10]. A stereotactic frame is used to localize and hit the target however, due to the non-availability of imaging in Gamma knife the accuracy is hampered. Gerbi et al. [11]. compared the mechanical accuracy of Gamma Knife and LINAC-based systems along with the dosimetric aspects including the target coverage and OAR doses and concluded that the LINAC-based stereotactic radiosurgery system can be an effective means of treating TN.
Over the past three decades due to the technological advancements of a linear accelerator (LINAC), it is possible to deliver a precise and fast radiation delivery with accurate imaging modality for Stereotactic radiosurgery (SRS) [12–15]. The treatment outcomes for TN patients with LINAC-based have been recently published and are comparable to that of Gamma knife. Several groups have reported their experience with Novalis Tx (Varian Medical Systems, Palo Alto, CA, USA) radiosurgery system for the treatment of trigeminal neuralgia [16–21]. The Novalis Tx system at our institute has 6MV SRS energy with 1,000 MU/min dose rate and on-board imager localization systems. It is equipped with BrainLab conical collimator cones ranging in diameter from 4 to 15 mm. BrainLab circular cones are made up of aluminium in brass shell (length=11.0 cm, outer diameter=6.5 cm, weight=5.3 kg) as shown in Figure 1A. We recently commissioned Varian LINAC-based SRS platform the Edge at our institute, which includes the standar d stereotactic accessory: conical cones and Varian head frame for frame- based SRS and a high definition multileaf collimator (HD-MLC). It contains 7 conical collimators of the following diameter sizes: 4, 5, 7.5, 10, 12.5, 15, and 17.5 mm. Varian circular cones are made up of tungsten in the brass shell (length=12.0 cm, outer diameter=7 cm, weight=7 kg) as shown in Figure 1B. The accelerator is equipped with two high-intensity modes (flattening filter free photons, 6XFFF and 10XFFF) with a maximum dose rate of 2,400 monitor units (MU) per minute for 10XFFF and 1,400 MU per minute for 6XFFF along with 6 MV flattened beam. The multiple imaging modalities for treatment localization, 2.5 MV portal images for verification, automatically triggered monoscopic kV imaging to track intrafractional motion and a Calypso/Varian electromagnetic beacon-based tracking system. It also contains 6D nonconductive couch top with rails (QFix kVue Calypso-compatible couch top) (QFix, Avondale, PA, USA) for precise patient setup. The system is also capable of doing frameless radiosurgery with an Optical surface monitoring system (OSMS). There are several advantages of FFF beams especially in SRS, SBRT due to the reduction in the treatment time hence impacting the patient motion and reduce patient discomfort. Due to the high number of monitor units involved in SRS the use of FFF beams may be most beneficial in circular collimator- or cone-based SRS treatments as it employs uncomfortable head frames or masks. The purpose of our study was to compare the dosimetric advantages of FFF beams for trigeminal neuralgia patients using 4 mm Varian conical collimators over previously treated patients with 6 MV SRS beam with BrainLab 4 mm cone. We compared the impact of FFF beam on Beam On time, Total number of MU’s in terms of delivery efficiency. We also compared the Gradient Index (GI), Homogeneity Index (HI), Doses to brainstem and Organ at risks (OAR’s) for 6X FFF and 6MV SRS beams.

(A) 4 mm BrainLab conical collimator, and (B) 4 mm Varian conical collimator.
Materials and Methods
A retrospective study was conducted consisting of a total of 5 TN patients (3 Right-sided and 2 Left-sided) who had been previously treated at our institution from 2009 to 2013 using frame-based, LINAC-based SRS on Novalis Tx. All patients underwent a high-resolution magnetic resonance imaging (MRI) scan consisting of 1 mm thin slices with T1-weighted, T2-weighted prior to treatment as per departmental protocol. An experienced Neurosurgeon placed the BrainLab stereotactic frame on patients head on the day of radiosurgery. The BrainLab stereotactic localizer was attached to the headring and patient was set up for the planning computerized tomography (CT) simulation which was performed on a 40 slice Siemens Biograph PET CT. CT images were acquired with 1 mm slice thickness following departmental SRS scanning protocol. The CT and MRI image registration was performed using the BrainLab stereotactic planning system and trigeminal nerve root (TNR) was delineated by an experienced radiation oncologist and neurosurgeon, for isocenter placement. The target was localized to the base of the trigeminal nerve at the junction of nerve entry and the brainstem which is approximately 3 mm from the edge of the brainstem. Organs at risk (OAR) were also delineated on the fused image datasets. For all the patients, 4 mm diameter cone was used for the treatment. A total of eight non-coplanar arcs plan were designed to deliver 80 Gy to the isocenter with a control dose of 50% isodose line using 6 MV SRS beam in iPlan BrainLab planning system as shown in Figure 2. In order to minimize brainstem dose all the plans were planned in such a way that the beam entry through the eyes was avoided. The maximum brainstem point dose was restricted to be less than 16 Gy. The dose calculation was based on Clarkson algorithm with a grid size for DVH calculation set to 1 mm.1), In the iPlan BrainLab TPS, a dose–volume histogram (DVH) was generated for all TN SRS treatment plans and same were evaluated by an experienced radiation oncologist, neurosurgeon, and medical physicist to ensure achievement of acceptable OAR doses. In addition to maximum dose to brainstem, the dose to 0.1 cc, 0.5 cc, and 1 cc of brainstem was also documented. All the approved plans were re-planned with 6X FFF in Eclipse Cone planning system (v13.6) module using Cone dose calculation (CDC) algorithm with a calculation grid size of 1 mm.2), All the plans used same beam geometry. The total number of monitor units along with the beam on time was compared for both Edge and Novalis Tx by redelivering the plans in QA mode of LINAC without patient to compare the delivery efficiency. Plan quality was evaluated by calculation of homogeneity index (HI=maximum dose/prescription dose) scores for the target and a Paddick gradient index (GI=50% isodose volume/100% isodose volume) score for each plan. The HI is a tool to analyze the uniformity of dose distribution in the target volume. The Gradient index is used to quantify the dose fall off. A plan with lower GI has a sharper average dose fall off from 100% to 50% isodose line [22]. Statistical analysis was performed using commercially available SPSS v17 (SPSS, Chicago, IL, USA). Comparison of beam on time (BOT), doses to brainstem, OAR’s, total monitor units, homogeneity index and gradient index analysis was performed using Mann Whitney U test with p-values<0.05 were considered to be statistically significant.
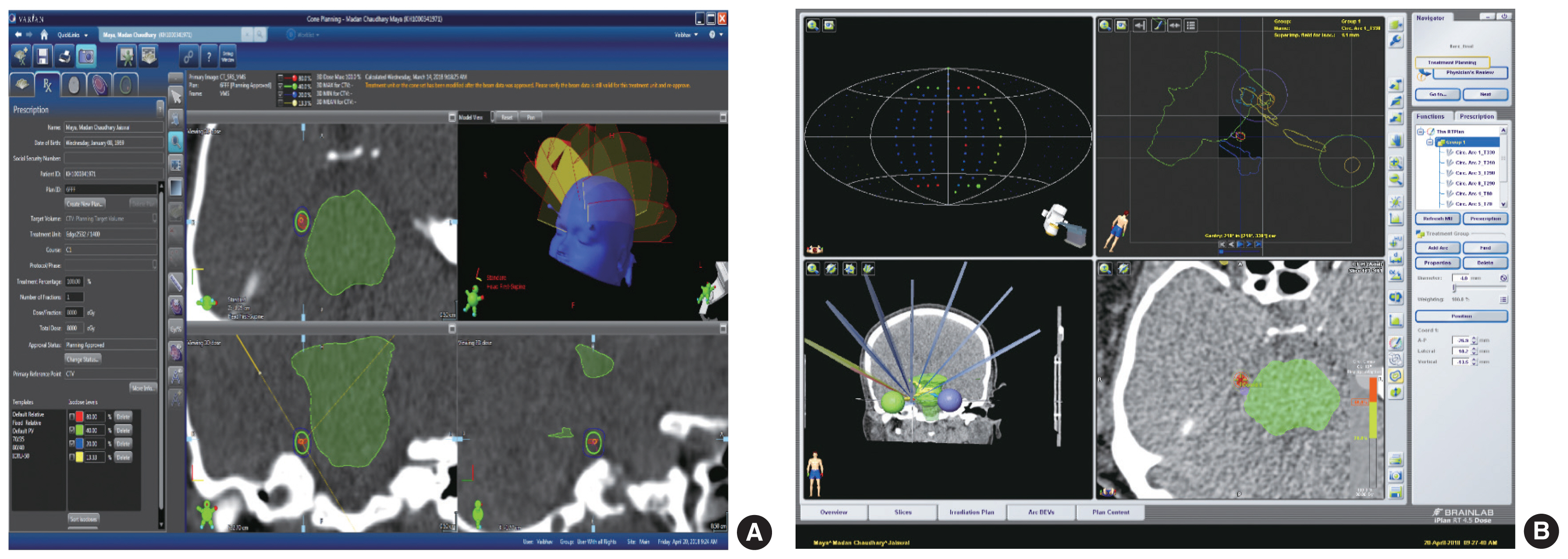
(A) Example of 8 arc arrangement in Eclipse Cone Planning module (6XFFF). (B) Example of 8 arc arrangement in iPlan BrainLab Planning system (6X SRS).
Results
The overall mean monitor units for all 5 patients were 19,869±543 for Edge LINAC when compared with 20,052± 889 for Novalis Tx as shown Table 1.

Percentage Variation of Beam on Time (BOT) for Edge and Novalis Tx
There was a significant difference in the average Beam On Time (BOT). The BOT for Edge was 14.22±0.26 minutes as compared with 19.72±1.1 minutes for Novalis Tx with an overall reduction of 28% using FFF beams for Edge LINAC. Table 1 shows the Beam ON time for 5 patients.
There was a signcant reduction of GI with Edge conical collimator with a median value 3.4±0.27 as compared with Novalis Tx conical collimator 4.17±0.20. A lower value indicated a sharp dose fall off beyond the target volume. No significant differences were found for HI. Table 2 show the comparative analysis of Gradient Index and Homogeneity Index for all the 5 patients.
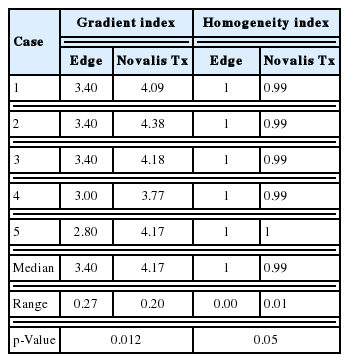
Gradient Index and Homogeneity Index Comparative Analysis
The maximum dose to the brainstem with Edge was 11 Gy with a median value 10.24±0.69 Gy ranged 9.3–11 Gy as compared with Novalis Tx the maximum dose was 14.8 Gy with a median value 14.28±0.33 Gy ranged 13.9–14.8 Gy. Table 3 show the doses received by brainstem for all the 5 patients.
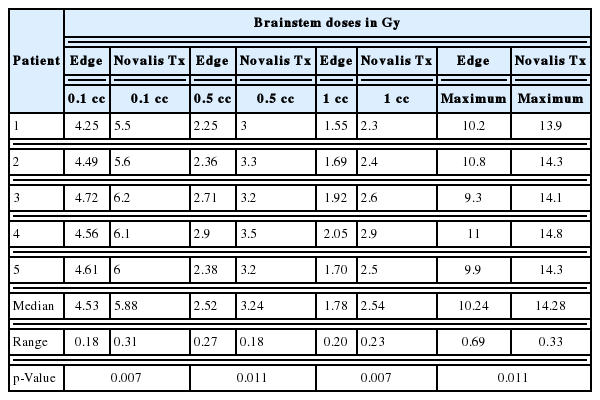
Dose Received by Brainstem for All the 5 Patients
Other organ at risks such as optic chiasm, optic nerve, and eye doses for both 6X FFF and 6X SRS beams are tabulated in Table 4. There was no significant difference between the doses received for both 6X FFF and 6X SRS beams.

Doses Received by OAR’s for All the 5 Patients
Discussion
There are several clinical studies on the treatment of TN with Gamma knife, Linear accelerator, and Cyber knife. However, there is no study till date on the comparison of FFF beams with FF beam for TN to our knowledge.
Pokhrel et al reported a detailed study for the treatment of TN with clinical outcomes for Novalis Tx with 27 patients and found that the average MU were 19,440±611, average BOT was 19.4±0.6 minutes and the maximum brainstem dose 15.9 Gy for an 80 Gy prescription. In our study, we were also able to achieve the same for Novalis Tx with average MU 19,869±543, average BOT 19.72±1.1 minutes and a maximum brainstem dose of 14.8 Gy [23]. There is only one study reported using Truebeam with FFF beams for the treatment of TN [24]. However, no dosimetric data was available to compare with the FFF beams for delivery efficiency.
In our study, we found that there was an overall 28% reduction of the beam on time when FFF beams are used for TN. Many investigators have already reported the utilization of Cyber knife for TN and the outcomes are comparable to LINAC-based SRS but with a longer average beam on time. The reduction of average BOT in FFF beams is an added advantage over Gamma Knife and Cyber knife treatments for TN [25–28]. Many studies have reported the advantage of using FFF beams for small target volumes in terms of treatment delivery and lower peripheral doses to OAR’s [29–34].
In our study, no statistically significant difference between 6X FFF and 6 MV SRS beam was found for HI. Regarding the dose gradient (GI), a statistical difference was found in our study. A lower GI value was reported in our study for 6X FFF beam using 4 mm Varian conical collimator. Hsu et al. compared the dosimetric comparison between Cone based LINAC, FFF VMAT LINAC, and tomotherapy for SRS and concluded that cone-based LINAC had the best dose gradient for tumours located near the critical organs such as brainstem [35]. The organ at risk in TN treatments is the brainstem which is very near to trigeminal nerve. Hence it is very important to restrict the brainstem dose as the most common complication associated with post-treatment of TN SRS is facial numbness [36]. The brainstem dose reported in our study with FFF beams was significantly less compared with 6 MV SRS beam with 28% reduction in maximum dose. One of the reasons for the reduction of brainstem dose was due to the design of Varian conical collimators in terms of the composition of material, weight and overall dimension. However, a detailed dosimetric study of both Varian and BrainLab conical collimator is needed which is beyond the scope of our study.
The evaluation of TN radiosurgery plan is based on the entrance distance of isodose line (IDL) into the brainstem hence the position of isocenter is defined on the IDL touching the brainstem [37]. There are many studies reported with different dose planning prescription techniques ranging from 90 Gy for the isocenter to nerve entry zone and 30% IDL is tangential to the brainstem and for 70 Gy, 40% IDL at the brainstem surface [38, 39]. There was a retrospective analysis done by Smith et al in 2011 for 179 patients on the outcomes of TN by varying the dose from 70 Gy to 90 Gy to the target and 30% isodose line touching the surface of brainstem for 70 Gy and 50% IDL for 90 Gy prescription. The results obtained with the 90 Gy were better than the 70 Gy with increased trigeminal dysfunction compared with low dose regimen. Our study being of a retrospective nature the follow up was beyond the scope. The dose received to the brainstem in our study indicates that the dose can be increased to 90 Gy due to the steep dose gradient received in FFF beams.Lema et al carried out a systematic search of TN literatures and suggested that there is a need for comparative studies due to the heterogeneity of the results and also suggested to conduct a study involving the planning of LINAC systems, fractionated treatment administration and application of radiosurgery without fixed stereotactic frame with the newest generation LINACS [40].
Our study has some potential limitations. Firstly, the small number of patients treated and retrospective analysis rather than randomize study. Additionally, due to the recent installation of this LINAC and rarity of this disease the clinical use of this technology for these diseases was very limited. There is a difficulty in evaluating and comparing the results of treatments of TN due to different dose strategies and hence there is a need of a uniform method for measuring the success of this disease. Future studies are planned to assess clinical outcomes and follow up along with the treatment efficiency for FFF beams.
Conclusion
The use of FFF beams for TN radiosurgery improves delivery efficiency with decreasing treatment time and the conical collimator of Edge linear accelerator reduces the dose to organ at risks. However, it is necessary to correlate the dose distribution with clinical outcomes and follow up is needed for long term clinical outcomes. The Edge linear accelerator can be effectively used for frame and frameless SRS. Further investigation is warranted with larger sample patient data.
Notes
Technical Reference Guide Rev.1.8 Brainlab Physics.
Eclipse Photon and Electron Algorithm Reference Guide.P1008611-002-B. December 2014.